Restoring perfusion through bone transport.
Transverse tibial transport moves a cortical bone window across the tibia, harnessing distraction-induced angiogenesis to recruit new blood supply for ischemic and diabetic lower-limb wounds.
End-stage ischemia
Non-reconstructable PAD cuts off blood supply to the foot. Wounds cannot heal without perfusion.
Failed revascularization
When bypass grafts and stents are not feasible or have failed, the vascular toolbox is exhausted.
Amputation as default
150,000 diabetes-related amputations occur annually in the U.S. — with 50–70% five-year mortality.
Distraction-induced angiogenesis
TTT harnesses the Ilizarov tension-stress principle: controlled mechanical strain on living tissue triggers regeneration and new blood vessel formation.
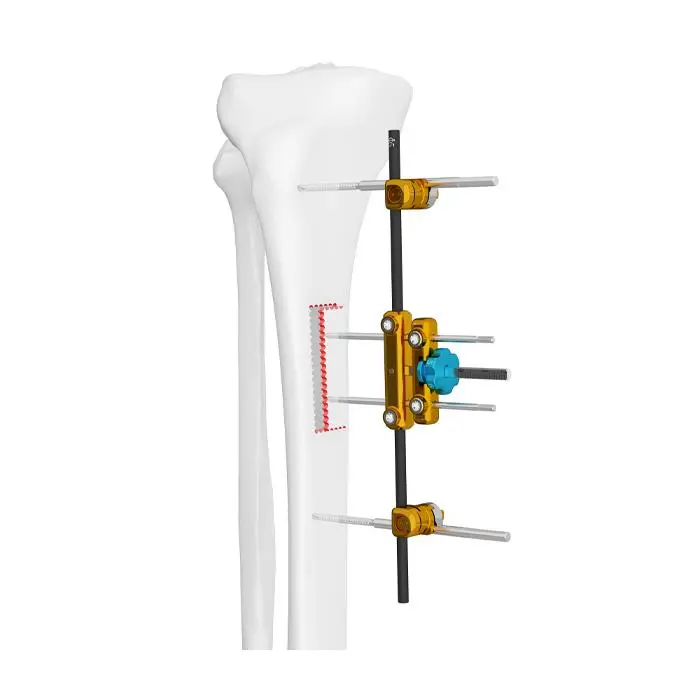
Osteotomy
A cortical bone window (~10 × 2 cm) is cut from the medial tibial surface, leaving periosteum intact on one side.
Transport
The bone window is moved laterally at ~1 mm/day using an external fixator. This stretches periosteum and soft tissue.
Angiogenesis
Mechanical strain upregulates VEGF, bFGF, and PDGF — driving formation of new collateral blood vessels across the distraction gap.
Perfusion
New vasculature restores blood flow distally. Ischemic wounds receive oxygen and nutrients, enabling healing.
Four phases of distraction-induced angiogenesis.
A cortical bone window is cut from the medial tibia and slowly transported laterally, then returned — triggering new blood vessel formation that restores perfusion to the ischemic limb.
A · Osteotomy
Two parallel cuts are made in the medial tibial cortex to define a rectangular bone window (~10 × 2 cm). The far cortex remains intact. The fixator is attached with pins through the bone window and anchoring pins above and below.
Published clinical evidence
The peer-reviewed literature supporting transverse tibial transport for limb salvage.
Multicenter cohort — 1,072 patients
The largest published TTT study: 1,072 patients across multiple Chinese centers with critical limb ischemia. 95% limb salvage rate. Established TTT as a viable biological revascularization strategy.
TTT with growth factor analysis
94.7% wound healing at 1 year. Demonstrated elevated serum VEGF and bFGF during the transport phase, confirming the angiogenic mechanism of action.
Tension-stress & skylight effects
Described the "Twin Open Skylight and Summon Effects" — the dual mechanism by which TTT creates both a periosteal stretch response and a bone-window gap that recruits vasculature.
Combined TTT + endovascular therapy
131 patients treated with TTT combined with endovascular intervention. Demonstrated that TTT can complement traditional vascular approaches for improved outcomes.
U.S. clinical guidelines for TTT
First published U.S. clinical guidelines for TTT application. 13-patient series establishing technique and protocol for American surgical practice.
Meta-analysis of TTT outcomes
Pooled analysis from multiple Chinese centers confirming high wound healing and limb salvage rates. Noted evidence is primarily retrospective; called for randomized controlled trials.
FDA-cleared devices for transverse bone transport.
Commercially available systems with regulatory clearance for TTT procedures.



XT3 System
Automated distraction system for both periosteal distraction and transverse tibial transport. Features a miniaturized, programmable motor that advances 0.031 mm/hour (0.75 mm/day). Used in the first fully automated tibial PD case (Feraru, Tan & Armstrong, IWJ 2026). FDA IDE approved for the SMILE-TTT pivotal trial — the first RCT outside China evaluating TTT for diabetic foot ulcers.
- Automated programmable motor — no manual adjustment needed
- Mini-rail fixator + distractor assembled together
- Used for both periosteal distraction and transverse tibial transport
- First automated PD case: toe pressure rose 22→50 mmHg, wound healed
- SMILE-TTT pivotal trial: 200 patients, multi-center RCT with Mount Sinai West
- NSF grant recipient (Dec 2024), ADA Innovation Challenge finalist (2025)


TrueLok Elevate
First commercially available device with a patented design specifically for transverse bone transport (TBT). Two-bar system with half pins and adjustment knob for transverse distraction and compression. Can be used standalone or in hybrid configuration with circular external fixator.
- Purpose-built for transverse bone transport
- Half pins D4mm to D6mm
- Standalone or hybrid with circular fixator (1–2 rings)
- 130+ procedures completed globally under limited market release
- Global commercial launch June 2025
- Active PMCF study: NCT07079774
Excelsior External Fixation System
Next-generation circular external fixation platform designed for limb salvage, incorporating tibial transverse transport (TTT) methodologies advanced from Chinese surgical innovations. Guided by the FASTR (Fixator Assisted Soft Tissue Repair) procedural framework for integrated bone and soft tissue management.
- Modular circular platform for bone transport and reconstruction
- FASTR framework for staged decision-making
- Addresses skeletal stability and soft tissue simultaneously
- FDA 510(k) cleared January 2026
- Named among "Six Orthopedic Startups to Track in 2026"
- Surgeon training: FASTR cadaver course (Miami, June 2026)
BFIX Transverse Bone Transport System
External fixator system specifically designed for transverse tibial bone transport. Compact design with anchor screws for tibial fixation and smaller screws for the cortical bone chip, with a turning nut for inward/outward transport of the bone segment.
- Purpose-built for TTT — compact unilateral design
- Two 20 mm anchor screws (1 mm dia.) for tibial fixation
- Two 10 mm screws (0.8 mm dia.) for cortical bone chip
- Turning nut for controlled inward/outward transport
- China Patent 201610722035.5
- Used in CAOS clinical guideline studies
Modular External Fixator
Modular external fixator system comprising threaded pins, adjusting nuts, combination clamps, and carbon fibre rods. Used in clinical research studies and finite element analysis of TTT safety.
- Modular design with carbon fibre rods
- Threaded pins + adjusting nuts + combination clamps
- Used in published TTT research studies
Adaptable Ring & Hybrid Fixation Systems
Standard Ilizarov-type circular frames and hexapod systems can be configured for TTT off-label. These include well-established platforms from major orthopedic device companies.
- Taylor Spatial Frame (TSF) — Smith+Nephew — hexapod, computer-guided
- TrueLok EVO & TL-HEX — Orthofix — ring fixation systems
- Standard Ilizarov frames — multiple manufacturers (JINLU, CZ Meditech, others)
- Cleared for fracture management; used off-label for TTT
Where the field is moving — events and active research.
Upcoming Events
Mt. Rushmore Diabetic Foot Reconstruction Forum
DFCon 2026
Active Clinical Trials
SMILE-TTT: BioDynamik XT3 Pivotal Trial
The limb-salvage ecosystem
Periosteal Distraction
The non-osteotomy alternative — PD elevates the periosteum without cutting bone. FDA 510(k) cleared.
periostealdistraction.com →Don't Amputate
Patient-facing resource for those told they need amputation. Learn about both PD and TTT, and find a specialist.
dontamputate.com →For Surgeons
Interested in offering TTT or PD to your patients? Contact us for clinical resources and training information.
An independent clinical resource
TibialTransport.com is an educational platform for surgeons and clinicians. Not affiliated with any device manufacturer. The information presented is drawn from peer-reviewed literature and is not medical advice.
Independent educational resource.
Not medical advice.